
The Canadian Scoliosis Screening Coalition
www.ScoliosisCanada.ca Site Map Contact us by email: CSSC@scoliosiscanada.ca
revised August 30, Oct 28, Nov 28, Dec 30, 2025, Feb 5, 9, 27, Mar 13, April 1 2026Signs of Scoliosis (AIS) every Canadian Parent should look for:
For children in the high risk age group in grades 5-7, every parent of children should learn the signs of scoliosis to look for and check their children. The age period to start checking for signs of Scoliosis (Adolescent Idiopathic Scoliosis, AIS) in your children is before puberty, girls age 10-12 years and boys age 13 or 14 1, which is when the AAOS, SRS, POSNA, and AAP advises screening to start by trained health professionals. Screening should take place one to two years BEFORE puberty and during puberty until skeletal maturity is reached and the child has finished growing. AIS is a genetic condition and runs in families so if there is a family history you might want to check earlier. Checking for signs of scoliosis can start at any age. AIS occurs more frequently in girls than boys and girls are 5-8X 2 at higher risk of developing curves that require treatment. Parents need to know that for girls with AIS, it has long been established that there is a higher risk of curve progression just before or at the age of menarche.
Perform a visual exam of your child by having them stand with their back towards you.
Because the spine can curve in different ways, the signs of Scoliosis (AIS) can be different from one child to the next. So a child may have one or more of the following signs below.
Signs of Scoliosis include:
Figure 14
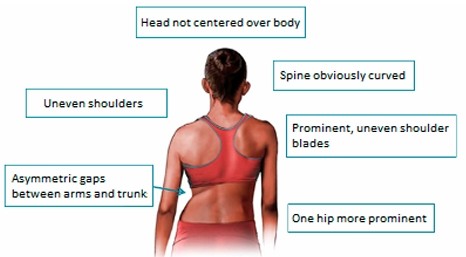
- The head is not centred over the body or tilts to one side.
- Uneven shoulders; one shoulder is higher than the other or
one shoulder blade is more prominent than the other. - Uneven hips; one hip is more prominent or lower than the other hip.
- Uneven waist creases or the waist appears uneven.
- Uneven space between hanging arms and the waist/trunk.
- Spine appears to curve and is not straight
- Changes in posture and walking gait.
- Clothes are not hanging evenly.
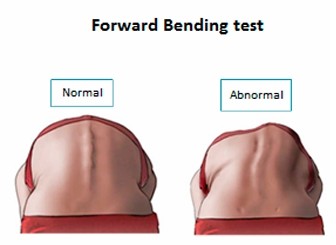
- Perform the Forward Bend Test (FBT) (aka Adams Forward Bend Test).
Have your child bend forward, legs straight and arms hanging freely, until their back is level with the floor and view their back from behind to see if both sides are the same. Check the waist, lower back and upper back to see if a ribcage or shoulder blade is protruding on one side. If the difference in height is more then 1 cm, your child may have Scoliosis.
More Screening Information & videos on Adolescent Idiopathic Scoliosis for Parents:
Watch How to detect Scoliosis at home, Explained under 1 minute from
Setting Scoliosis Straight Foundation (US non-profit established by surgeons)
For more information,
Adolescent Idiopathic Scoliosis
from the non-profit UK Scoliosis Support & Research.
Information on Scoliosis from
Boston's Children's Hospital
Watch the SRS Educational Videos: Scoliosis Screening Exam and
Use of a Scoliometer
Or watch How To Use A Scoliometer To Measure Scoliosis Curve Rotation and Monitor For Progression from a Physiotherapist at Align Therapy
PRINT a downloadable PDF brochure from non-profit Scoliosis Alberta Society
Scoliosis Screening Brochure
For information on Scoliosis from the Scoliosis Research Society (SRS) refer to:
Diagnosis & Screening of Scoliosis FAQ
Watch the Scoliosis Video Handbook chapters from (US non-profit) Setting Scoliosis Straight Foundation
Video Channel of Setting Scoliosis Straight
Note: none of the above North American or UK (like Canada they stopped screening in the 1980s) sites promotes Schroth Physiotherapeutic Scoliosis-Specific Exercises PSSE as a conservative treatment for mild curves and practice 'observation only'. Except
here:
Columbia University Irvine Medical Center Comprehensive patient resources: What is Scoliosis, different types, treatments, diagnostics and more.
And read here about
The Schroth Method from John Hopkins Health.
Early diagnosis and treatment is key, so if you are concerned your child has Scoliosis, please make an appointment for your child as soon as possible with your primary care provider or child's pediatrician or nurse practitioner. He or she may order x-rays of your child's entire spine to confirm
a diagnosis and refer your child to a paediatric orthopaedic spine surgeon at a children's hospital who specializes in spinal deformities and Scoliosis, or the Scoliosis clinic at the closest children's hospital. Children with mild to moderate scoliosis curves may be treated by Advanced Practice Physiotherapists and Nurse Practitioners specialized in scoliosis at children's hospital scoliosis clnics, in a collaborative team environment.
The x-rays will be read by a specialist to measure the degree of your child's spinal curve which is called the COBB angle. Scoliosis is defined by a COBB angle that is greater than 10° . Curves under 20° Cobb angle are considered mild.
(
WHY THIS MATTERS:
Public health in Canada does not screen children for common Scoliosis (AIS) nor rare diseases. And awareness is low among primary care providers.
It is critically important to recognize that children (and young adults) with these rare genetic/heritable connective tissue disorders — are at
WHERE TO FIND HELP please click on ==> Links to resources and references on HCTDs. Please watch Family of woman who died after undiagnosed Marfan syndrome speaks out CTV News, Toronto News, Jan 7, 2026 and the Ontario family's Federal Petition advocating screening for rare diseases. Early cardiac diagnosis is critical and preventative treatment can be life-saving. )
PARENTS MUST BE MADE AWARE AND INFORMED of a recent study from Toronto Sickkids,
Kim DJ, Dermott JA, Mitani AA, Doria AS, Howard AW, Lebel DE. The diagnostic accuracy of community spine radiology for adolescent idiopathic scoliosis brace candidates
Eur Spine J. 2024 Oct;33(10):3776-3783. doi: 10.1007/s00586-024-08389-1. Epub 2024 Jul 17. PMID: 39014076.
Please know, for the majority of children, Scoliosis curves are mild and remain mild and do not cause health problems and according to studies mild curves do not cause pain for most children but can cause lower back pain for some children with lumbar curves11 . But for some children Scoliosis, can lead to progressive curves that left undetected and untreated can lead to serious long-term health problems such as chronic back pain, respiratory issues, physical deformity, decreasing physical functioning, and psychosocial distress. Early-detection, diagnosis and early-treatment is critically important as during puberty for a small number of children curves can progress rapidly during growth spurts.
Treatments available for Scoliosis:
In North America. the standard of care has been for decades, one, for children with mild scoliosis curves are observed and monitored with x-rays at regular check-ups during growth, two they can be prescribed orthotic brace treatment for mild to moderate curves and wear a brace, fitted with new custom braces as they grow (much like buying new shoes for your child) until they are finished growing, or three, surgery is prescribed to correct and stop the curve progression for children with severe curves. The Canadian Scoliosis Screening Coalition is advocating that children with mild curves be offered conservative treatment with scoliosis-specific physiotherapy, as in Europe and now China, which has been documented to stop and correct mild curves in growing children and to add it as an adjunct treatment to orthotic bracing as studies have shown it increases the success rate of orthotic bracing to stop the progression of curves for over 70% of children.
For educational information and patient videos on bracing click on Bracing from the Scoliosis Research Society.
From Toronto Sickkids Hospital What to expect from the Orthotics Clinic after a referral. and the very informative Scoliosis Bracing how does it work? from CHU Sainte-Justine of Montreal.
For some children, with moderate to severe curves and who are still growing, newer growth-friendly surgeries may be offered at some children's hospitals that corrects the curvature and no permanent implanted rods or screws fuse the spine, which restricts some movement of the spine. And the child is left with a more natural and flexible spine. The gold standard of surgery for treating severe curves is fusion to prevent curve progression and correct the deformity. All spine surgeries are invasive and carry risks and complications. But the complication rates are higher with the newer growth-friendly surgeries.
Note, if your chiid is a mature teenager who has completed growing and reached skeletal maturity, than conservative non-operative treatments of Schroth physiotherapy and Orthotic Bracing will likely be unsuccessful to correct curve deformity as the spine is no longer flexible.
Children diagnosed with AIS are exposed to radiation with repeated x-rays and have a slightly higher risk of cancer. However, many children's hospitals now have low-dose radiation 3D scanners called EOS that have signficantly reduced radiation and lessons the risk to cancer.
Screening and Monitoring Tools:
If you child has been diagnosed with Scoliosis by a physician and is still growing between 10-15 years, you may wish to purchase one of the following tools that health practitioners use,
- Scoliometer -inexpensive (used for decades by clinicians world-wide) measuring tool that costs less then $20 online. As well,
digital Scoliometer APPS exist for smart phones that can be purchased online.
Recommended by the Scoliosis Research Society (SRS) in their 2015 Position Statement on Screening for health professionals to use as a 2nd step in conjunction with the Forward Bend Test. Measures the degree of spinal deformity of the spine called 'trunk rotation', while doing the Forward Bend test. The reading
has to be at least
5-7o degrees for a Scoliosis diagnosis. The tool is similar to a carpenter's level. -
Momentum Spine A digital smartphone APP that utitizes high-quality smartphone video/cameras, where parents at home can screen their child in 45 seconds. Provides
radiation free monitoring and produces a comparableclinical-grade 3-D spine scan . Works with AI software that "assesses your degree (cobb angle) of curvature, helps you track curve progression over time and automatically calculates key body measurements like shoulder asymmetry, trunk shift and height growth. The mobile app also directs you to custom-made educational content specifically designed for different scoliosis curve types. You can also seamlessly share your data and 3D Models with your care team...". This smartphone APP provides a platform capability ofremote monitoring between patients and spine specialists and hospitals. With the great potential to reduce visits (and healthcare costs) to hospital clinics, and identify the need for early intervention faster for spine specialists and hospitals. Recommended by top US spine specialists. HIPAA compliant, Health Canada and FDA approved. Available by prescription or OTC purchase online through Apple App Store and Google Playstore. Currently only available in Canada and the US. As of Sept 1, 2025 compatible with: iPhone 11 and newer models (excluding iPhone SE.), Samsung S23 and newer models, Google Pixel 6 and newer models, Galaxy Note 5 and newer models. (NOTE: 12/2025 Two Canadian clinical trial studies 1,5 reported Momemtum APP's AI processed Cobb angle measurement produced a mean average degree of error of 4.05° - 6.2° when compared to same-day hospital radiographic imaging (x-rays) but within acceptable levels of variability between clinicians and "can be used to detect and monitor adolescent idiopathic scoliosis remotely" and "facilitates frequent at-home remote monitoring...to avoid unnecessary hospital visits and spinal x-rays, potentially detecting early curve progression as well") -
Romano, M., Mastrantonio, M. Torsion bottle, a very simple, reliable, and cheap tool for a basic scoliosis screening. ScoliosisJournal 13, 4 (2018). https://doi.org/10.1186/s13013-018-0150-6, distributed under Creative Commons license.
'A simple tool (the torsion bottle) that can be made at home with a 500 ml plastic water bottle, the aim of this study was to offer an instrument for home use by parents in low-income countries and those in remote areas with no access to a scoliometer or online digitial screening APPs and lack of access to health professionals.' Directions provided.
Common Myths and Misinformation about Adolescent Idiopathic Scoliosis:
- You did not drink enough milk or eat the right foods. Scoliosis is a genetic condition that runs in families. It is not caused by anything a child or parent did or did not do. But all children require a healthy diet that includes calcium and vitamin D in their daily diet for good bone health. 10,12
- Bad posture or slouching does not cause scoliosis (but can cause kyphosis later in life).
- Heavy backpacks do not cause scoliosis (but should not weigh more then 10-15% of the body weight of a child).
- Swimming does not cause scoliosis.
- Gymnastics, Ballet and/or Rhythmic gymnastics does not cause scoliosis.
- Scoliosis (Adolescent Idiopathic Scoliosis (AIS)) does not make a person fragile.
- Scoliosis (AIS) will not restrict anyone (males or females) from having a family but since it is a genetic condition, it is important to closely monitor children where there is a family history of scoliosis and screen early.26
- Scoliosis (AIS) is not a girls only disease. Boys can get it too. But it occurs more often in girls and girls are at much higher risk 5-8X of developing severe curves that require treatment.
- Scoliosis does not cause back pain. This is untrue. But during childhood the majority of children with scoliosis of mild to moderate curves according to studies do not suffer back pain any different from children without scoliosis. But children with lumbar curves can suffer from back pain. And most children with severe Scoliosis curves of all types report or feel significant back pain. And later in life untreated scoliosis can cause back pain and other health problems.
WHERE TO FIND HELP ==> Canadian Directory of Paediatric Clinical Scoliosis Resources
References:
Note, the following references are publications and studies primarily meant for health professionals. Note: the two top professional societies established for the treatment of Adolescent Idiopathic Scoliosis and Spinal Deformities are the Scoliosis Research Society (SRS), which includes over 1,000 of the world's leading spine surgeons, researchers, physician assistants and orthotists who are involved in research and treatment of spinal deformities. And SOSORT, the International Society on Scoliosis Orthopaedic and Rehabilitation Treatment. SSORT is a non-profit International society of Doctors, Physical Therapists. Orthotists and Psychologists formed in 2003 for Scoliosis care whose focus is on non-operative care,
- Position Statement Screening for the Early Detection of Idiopathic Scoliosis in Adolescents by The Scoliosis Research Society (SRS), American Academy of Orthopaedic Surgeons (AAOS), Pediatric Orthopaedic Society of North America (POSNA), and American Academy of Pediatrics (AAP).
- Negrini S, Donzelli S, Aulisa AG, Czaprowski D, Schreiber S, de Mauroy JC, Diers H, Grivas TB, Knott P, Kotwicki T, Lebel A, Marti C, Maruyama T, O'Brien J, Price N, Parent E, Rigo M, Romano M, Stikeleather L, Wynne J, Zaina F. 2016 SOSORT guidelines: orthopaedic and rehabilitation treatment of idiopathic scoliosis during growth. Scoliosis Spinal Disord. 2018 Jan 10;13:3. doi: 10.1186/s13013-017-0145-8. PMID: 29435499; PMCID: PMC5795289.
- Grivas TB, Vasiliadis E, Mazioti C, Mamzeri A, Papagianni D, Katzouraki G, Sekouris N.
To Screen or Not to Screen: "False Positive" Cases-Can They Be Treated as Definitely False? Properly Selecting the Screening Age-Range Groups in Scoliosis Screening Programs. Healthcare (Basel). 2025 Mar 10;13(6):600. doi: 10.3390/healthcare13060600. PMID: 40150450; PMCID: PMC11942112."... Today, evidence demonstrates that signs and symptoms of scoliosis can be significantly improved through intensive inpatient exercise programs...
It is also well-documented and widely accepted that bracing alters the natural course of IS ...and that SSS programs reduce the number of patients requiring surgical intervention...Conclusions
One reason SSS programs have been discontinued is the occurrence of false positive cases. Many younger children are referred from these programs due to trunk asymmetry but actually have a straight spine or a Cobb angle below 10 degrees, leading to their classification as “false positives”. However, it is highly likely that some of these children may later develop IS as they grow, meaning they should not be definitively labeled as false positives...The recommended age group for screening is adjusted based on latitude, as the timing of menarche varies accordingly. It is advised to conduct screenings within a window of two years before and two years after the average age of menarche in a given country. Ultimately, SSS programs are strongly recommended due to their numerous benefits."
- de Groot C, Heemskerk JL, Willigenburg NW, Altena MC, Kempen DHR. Educating Parents Improves Their Ability to Recognize Adolescent Idiopathic Scoliosis: A Diagnostic Accuracy Study. Children (Basel). 2022 Apr 15;9(4):563. doi: 10.3390/children9040563. PMID: 35455607; PMCID: PMC9025014."...Conclusions: This study showed that the education of parents improved their ability to detect scoliosis from 68.8% to 74.0%, without increasing the false positive referral rate...education can improve the awareness and ability to detect scoliosis, but will not replace screening by professionals. Education of the parents could be a strategy to facilitate adequate referral of patients with scoliosis to a physician in healthcare systems without professional screening."
- Konieczny MR, Senyurt H, Krauspe R. Epidemiology of adolescent idiopathic scoliosis. J Child Orthop. 2013 Feb;7(1):3-9. doi: 10.1007/s11832-012-0457-4. Epub 2012 Dec 11. PMID: 24432052; PMCID: PMC3566258.
- Ogata, Yosuke et al. Timeline of curve progression around menarche in small adolescent idiopathic scoliosis curves without influence of braces: a single-center longitudinal cohort study of 1,090 patients The Spine Journal, 0 Volume 0, Issue "...Menarche is widely recognized as one of the prognostic factors for curve progression in patients with adolescent idiopathic scoliosis (AIS)..."
- Curve Progression in Untreated Patients with Scoliosis (AIS) from the Scoliosis Research Society Education Resource Center. See table 1. "...Studies have consistently shown the more skeletally immature a patient is, the greater the chance of progression. It also shown the larger the curve at presentation, the higher the probability of progression of the deformity. There is also a greater risk of progression before the onset of menarche in females..."
- Mao SH, Jiang J, Sun X, Zhao Q, Qian BP, Liu Z, Shu H, Qiu Y. Timing of menarche in Chinese girls with and without adolescent idiopathic scoliosis: current results and review of the literature. Eur Spine J. 2011 Feb;20(2):260-5. doi: 10.1007/s00586-010-1649-6. Epub 2010 Dec 14. PMID: 21153847; PMCID: PMC3030718. "...Age at menarche is closely related to scoliosis progression during adolescence..."
- Paranjape CS, Welborn MC. Spine health: Back pain and deformity progression. J Pediatr Soc North Am. 2024 Apr 10;7:100062. doi: 10.1016/j.jposna.2024.100062. PMID: 40433264; PMCID: PMC12088328. "...Back pain is highly prevalent affecting up to a third of adolescents and is even more so in patients who are vitamin D deficient.(2)Scoliosis patients from various etiologies all experience higher rates of back pain and tend to have lower bone mineral density than their healthy pediatric peers.(3)There is an interplay between deformity and bone health, where deformity can both drive and be driven by bone health.(4)Treatments targeting bone health may positively affect both natural history and surgical outcomes for patients who have scoliosis with various underlying etiologies.(5)Further research is needed to elucidate mechanistic pathways that link bone health to deformity and to evaluate targets for therapy..."
- Minkowitz B, Spingarn CM. Effective counseling for children's bone health. J Pediatr Soc North Am. 2024 Apr 10;7:100032. doi: 10.1016/j.jposna.2024.100032. PMID: 40433273; PMCID: PMC12088366.
Key ConceptsBone health needs to be prioritized from a young age because the majority of peak bone mass is attained by the end of the second decade of life.- Patient counseling and patient buy-in are imperative to create lasting impact.
- Bone health is a recipe and the amounts of ingredients needed will vary according to growth and body size.
- Vitamin D dosing should take weight and body mass into consideration to achieve optimal serum levels.
- Balioglu MB, Aydin C, Kargin D, Albayrak A, Atici Y, Tas SK, Kaygusuz MA. Vitamin-D measurement in patients with adolescent idiopathic scoliosis. J Pediatr Orthop B. 2017 Jan;26(1):48-52. doi: 10.1097/BPB.0000000000000320. PMID: 27089048."...Vitamin-D levels were lower in the AIS group, with no sex-specific effects, indicative of a possible vitamin-D resistance in AIS. Vitamin-D levels correlated positively with Ca levels and negatively with Cobb’s angle, indicative of a possible role of vitamin D in the etiopathogenesis of AIS.
Patients with AIS should be monitored for vitamin-D deficiency/insufficiency ..."- Tsz Ping Lam 1, , Benjamin Hon Kei Yip 2, , Gene Chi Wai Man 1, , Wayne YW Lee 1, , Elisa Man Shan Tam 1, , Kwong Man Lee 1, , Fiona Wai Ping Yu 1, , Bobby Kin Wah Ng 1, & Jack Chun Yiu Cheng 1,Effective therapeutic control of curve progression using calcium and vitamin D supplementation for adolescent idiopathic scoliosis – a randomized double-blinded placebo-controlled trial Bone Abstracts (2017) 6 OC8 | DOI: 10.1530/boneabs.6.OC8 "...Conclusion:
The results of this study provide strong evidences that calcium+Vit-D supplementation can improve bone strength in AIS . Its therapeutic effect on preventing curve progression is correlated with increase in FEA parameters, low baseline 25(OH)Vit-D level and low baseline dietary calcium intake.- Herdea A, Dragomirescu MC, Ulici A, Lungu CN, Charkaoui A. Controlling the Progression of Curvature in Children and Adolescent Idiopathic Scoliosis Following the Administration of Melatonin, Calcium, and Vitamin D. Children (Basel). 2022 May 21;9(5):758. doi: 10.3390/children9050758. PMID: 35626935; PMCID: PMC9140159."Abstract...In this perspective, randomized, case-control, interventional study, the impact of using melatonin, calcium, and vitamin D, respectively, on idiopathic scoliosis patients was analyzed. Our preliminary results showed that these drugs positively affected the illness progression quantified by the spine curvature.
Patients with idiopathic scoliosis may benefit from a novel treatment by supplementation with vitamin D, calcium, and melatonin ....The treatment of childhood and adolescent idiopathic scoliosis follows the guidelines based on Cobb angle and other factors such as age, gender, or menarche status for girls. The staging of treatment includes physiotherapy, wearing a brace, and surgery for advanced cases. None of these steps takes into account the possible existence of a metabolic factor that aggravates the evolution of the disease...."- Beauséjour M, Aubin D, Fortin C, N'dongo Sangaré M, Carignan M, Roy-Beaudry M, Martinez C, Bourassa N, Jourdain N, Labelle P, Labelle H. Parents can reliably and accurately detect trunk asymmetry using an inclinometer smartphone app. BMC Musculoskelet Disord. 2022 Aug 5;23(1):752. doi: 10.1186/s12891-022-05611-3. PMID: 35932044; PMCID: PMC9354306. (Note, inclinometer is another name for Scoliometer)
- Siwiec A, Domagalska-Szopa M, Kwiecień-Czerwieniec I, Dobrowolska A, Szopa A. Impact of Idiopathic Scoliosis on the Cardiopulmonary Capacity of Adolescents. J Clin Med. 2024 Jul 28;13(15):4414. doi: 10.3390/jcm13154414. PMID: 39124681; PMCID: PMC11312811. “Conclusion: Children and adolescents with mild-to-moderate scoliosis during CPET exhibited a lower ventilation capacity and lower VO2max than age-matched healthy adolescents. Furthermore, lower ventilation capacity and lower VO2max may be responsible for reduced exercise tolerance in adolescents with mild-to-moderate IS and the CRF parameters of children with mild-to-moderate scoliosis are not dependent upon the Cobb or rotation angles of the primary spinal curvature. Physiotherapy and physical activity should be recommended to prevent cardiorespiratory failure in later life in patients with scoliosis....”
- Sarkovich S, Leonardi C, Darlow M, Martin D, Issa P, Soria T, Bronstone A, Clement C. Back pain in adolescent idiopathic scoliosis: frequency and risk factors. Spine Deform. 2024 Sep;12(5):1319-1327. doi: 10.1007/s43390-024-00904-0. Epub 2024 Jun 23. PMID: 38910187; PMCID: PMC11344019 "Among those who reported back pain, 63.2% specified a location with the majority reporting pain in the lumbar region (56%) and, less commonly, in the thoracic (39%) and scapular (8%) regions. Lumbar pain was associated with significantly higher pain intensity (p = 0.033).... Nearly half (48%) of newly diagnosed AIS patients experience back pain which is higher than the prevalence of 33% seen in the general adolescent population. Pain was more prevalent among patients over the age of 13, with heavier body weight... Pain was most commonly reported in the lumbar region, especially among patients with lumbar curves....
- Makino T, Kaito T, Sakai Y, Takenaka S, Yoshikawa H. Health-related Quality of Life and Postural Changes of Spinal Alignment in Female Adolescents Associated With Back Pain in Adolescent Idiopathic Scoliosis: A Prospective Cross-sectional Study. Spine (Phila Pa 1976). 2019 Jul 15;44(14):E833-E840. doi: 10.1097/BRS.0000000000002996. PMID: 30817729.
- Wong AYL, Samartzis D, Cheung PWH, Cheung JPY. How Common Is Back Pain and What Biopsychosocial Factors Are Associated With Back Pain in Patients With Adolescent Idiopathic Scoliosis? Clin Orthop Relat Res. 2019 Apr;477(4):676-686. doi: 10.1097/CORR.0000000000000569. PMID: 30516661; PMCID: PMC6437349.
- Théroux J, Le May S, Hebert JJ, Labelle H. Back Pain Prevalence Is Associated With Curve-type and Severity in Adolescents With Idiopathic Scoliosis: A Cross-sectional Study. Spine (Phila Pa 1976). 2017 Aug 1;42(15):E914-E919. doi: 10.1097/BRS.0000000000001986. PMID: 27870807."...Conclusion: Spinal pain is common among patients with AIS, and greater spinal deformity was associated with higher pain intensity. These findings should inform clinical decision-making when caring for patients with AIS...."
- Théroux J, Stomski N, Hodgetts CJ, Ballard A, Khadra C, Le May S, Labelle H. Prevalence of low back pain in adolescents with idiopathic scoliosis: a systematic review. Chiropr Man Therap. 2017 Apr 20;25:10. doi: 10.1186/s12998-017-0143-1. PMID: 28439404; PMCID: PMC5399433."Conclusion: The results of this systematic review indicate that adolescents with idiopathic scoliosis frequently experience low back pain...."
- Sato T, Hirano T, Ito T, Morita O, Kikuchi R, Endo N, Tanabe N Back pain in adolescents with idiopathic scoliosis: epidemiological study for 43,630 pupils in Niigata City, Japan. Eur Spine J. 2011 Feb;20(2):274-9. doi: 10.1007/s00586-010-1657-6. Epub 2010 Dec 17. PMID: 21165657; PMCID: PMC3030705. “...Scoliosis group experienced significantly more severe pain, and of a significantly longer duration with more frequent recurrences in comparison to No scoliosis group.
- G Bisson D, Lama P, Abduljabbar F, Rosenzweig DH, Saran N, Ouellet JA, Haglund L. Facet joint degeneration in adolescent idiopathic scoliosis. JOR Spine. 2018 May 24;1(2):e1016. doi: 10.1002/jsp2.1016. PMID: 31463443; PMCID: PMC6686828. “...AIS facet joint cartilage shows hallmarks of OA including proteoglycan loss, overexpression of pro-inflammatory mediators, increased synthesis of matrix-degrading proteases and fragmentation of SLRPs. As with patients with age-related OA, the premature joint degeneration seen in scoliotic patients is likely to contribute to the pain perceived in some individuals....”
- Paramento M, Passarotto E, Maccarone MC, Agostini M, Contessa P, Rubega M, Formaggio E, Masiero S. Neurophysiological, balance and motion evidence in adolescent idiopathic scoliosis: A systematic review. PLoS One. 2024 May 22;19(5):e0303086. doi: 10.1371/journal.pone.0303086. PMID: 38776317; PMCID: PMC11111046. “We found significant evidence of
impaired standing balance in individuals with AIS who greatly rely on visual and proprioceptive information to stay upright...Bracing appears to be an effective treatment for AIS, leading to improvements in static balance and gait..."- Serhan, Karolina A. MD1; Abraham, Vivek M. MD1; Shirley, Eric D. MD1,a. The Impact of Adolescent Idiopathic Scoliosis on Pregnancy. The Journal of Bone and Joint Surgery 107(7):p 771-777, April 2, 2025. | DOI: 10.2106/JBJS.24.00850
"Abstract: ➢ Physiologic changes during pregnancy alter the biomechanics of the spine, including increased ligamentous laxity, lumbar lordosis, and pelvic tilt. ➢ Patients with adolescent idiopathic scoliosis treated with a fusion construct with the lowest instrumented vertebra of L3 and below have an increased risk of developing low back pain during pregnancy. ➢ There is a low risk of curve progression during pregnancy for patients with adolescent idiopathic scoliosis treated with spinal fusion. ➢ Although neuraxial anesthesia is possible in patients who had previously undergone spinal fusion for adolescent idiopathic scoliosis, successful placement may require a more experienced provider and more attempts to place the epidural."
- Normand É, Franco A, Parent S, Lombardi G, Brayda-Bruno M, Colombini A, Moreau A, Marcil V. Association between the GLP1R A316T Mutation and Adolescent Idiopathic Scoliosis in French Canadian and Italian Cohorts Genes (Basel). 2024 Apr 11;15(4):481. doi: 10.3390/genes15040481. PMID: 38674415; PMCID: PMC11050147. "...To date, several genetic variants have been associated with AIS. The identified associated genes are involved in conjunctive tissue structures, growth and puberty, bone formation, metabolism, melatonin pathway, and ciliary functions...Our results support that the GLP1R A316T polymorphism is associated with a higher risk of developing AIS, but without being associated with disease severity and progression....”
- Zloof Y, Ankory R, Braun AE, Braun M, Abuhasira S, Schwartz N, Yaari D, Glassberg E, Shlaifer A. The Hereditary Nature of Adolescent Spinal Deformities: A Study of Over 600,000 Adolescents. Spine (Phila Pa 1976). 2022 Jun 15;47(12):841-846. doi: 10.1097/BRS.0000000000004355. Epub 2022 Apr 21. PMID: 35472202.
“...Results... the odds ratios (OR) for ASD among adolescents whose father, mother, or both parents had spinal deformity were 1.46, 1.74, and 2.58, respectively ..." (note: ASD, Adolescent Spinal Deformity includes Adolescent Idiopathic Scoliosis)- Baschal EE, Terhune EA, Wethey CI, Baschal RM, Robinson KD, Cuevas MT, Pradhan S, Sutphin BS, Taylor MRG, Gowan K, Pearson CG, Niswander LA, Jones KL, Miller NH.Idiopathic Scoliosis Families Highlight Actin-Based and Microtubule-Based Cellular Projections and Extracellular Matrix in Disease Etiology. G3 (Bethesda). 2018 Jul 31;8(8):2663-2672. doi: 10.1534/g3.118.200290. PMID: 29930198; PMCID: PMC6071588. “Idiopathic scoliosis (IS) is a structural lateral spinal curvature of ≥10° that affects up to 3% of otherwise healthy children and can lead to life-long problems in severe cases. It is well-established that IS is a genetic disorder..."
- Zhu Z, Xu L, Qiu Y. Current progress in genetic research of adolescent idiopathic scoliosis.Ann Transl Med. 2015 May;3(Suppl 1):S19. doi: 10.3978/j.issn.2305-5839.2015.02.04. PMID: 26046064; PMCID: PMC4437942. “...Recently, two genome-wide association studies of AIS performed in Japan revealed that ladybird homeobox 1 (LBX1) gene and G protein–coupled receptor 126 (GPR126) gene could play a role in the etiopathogenesis of the disease. Since
the association between these two genes and AIS were successfully validated in the Caucasian and the Chinese population , LBX1 gene and GPR126 gene were the most reliable genetic variants underling the development of AIS.”- Labelle H, Richards SB, De Kleuver M, Grivas TB, Luk KD, Wong HK, Thometz J, Beauséjour M, Turgeon I, Fong DY. Screening for adolescent idiopathic scoliosis: an information statement by the Scoliosis Research Society international task force.Scoliosis. 2013 Oct 31;8:17. doi: 10.1186/1748-7161-8-17. PMID: 24171910; PMCID: PMC3835138. “...Adolescent idiopathic scoliosis (AIS) is a complex 3-D deformation of the trunk, with a prevalence of 2-4%. Among patients with AIS, 8% to 9% will be treated by brace and 0.1% will need surgery using spinal instrumentation and fusion...TF members agreed that the recommended threshold for the use of the scoliometer should be between 5° and 7° when used alone...members agreed that screening should be conducted two years before onset of menses. ..After a critical review of the available evidence, the SRS International Task Force on Scoliosis screening, supported by the SRS Board of Directors, makes the following statements and recommendations regarding scoliosis screening:...Scoliosis screening is recommended as valuable in the following domains: technical efficacy, clinical, program and treatment effectiveness...”
- Liang ZT, Guo CF, Li J, Zhang HQ. The role of endocrine hormones in the pathogenesis of adolescent idiopathic scoliosis. FASEB J. 2021 Sep;35(9):e21839. doi: 10.1096/fj.202100759R. PMID: 34387890. ”...Accumulating evidence shows that the abnormal levels of many hormones including estrogen, melatonin, growth hormone, leptin, adiponectin and ghrelin, may be related to the occurrence and development of AIS. The purpose of this review is to provide a summary and critique of the research published on each hormone over the past 20 years, and to highlight areas for future study...”
- Lee CF, Fong DY, Cheung KM, Cheng JC, Ng BK, Lam TP, Yip PS, Luk KD. A new risk classification rule for curve progression in adolescent idiopathic scoliosis. Spine J. 2012 Nov;12(11):989-95. doi: 10.1016/j.spinee.2012.05.009. Epub 2012 Jun 21. PMID: 22727318. "...Results The new classification rule identified four risk groups of curve progression. Patients with a curvature of 26° and more and less than 18° constituted the highest and lowest risk groups, respectively. The two intermediate groups were identified by the age (11.3 years), menarcheal status, and body height (154 cm)... Conclusions The risk classification rule only uses information at the first presentation and can aid physicians in deriving an efficient management.
- Yang, Y., Chen, Z., Huang, Z. et al. Risk factors associated with low bone mineral density in children with idiopathic scoliosis: a scoping review. BMC Musculoskelet Disord 24, 48 (2023). https://doi.org/10.1186/s12891-023-06157-8 "...This scoping review showed that BMD was generally lower in children with IS than in asymptomatic controls. Genetic, endocrine, and lifestyle-related factors might be associated with low BMD in children with IS. Bone synthesis or absorption may be directly regulated by endocrine factors, while genetic and lifestyle-related factors may influence BMD via the endocrine pathway. Comprehensive screening for low BMD risk factors may be reasonable to prevent osteoporosis and progression in children with IS....
- Rose LD, Williams R, Ajayi B, Abdalla M, Bernard J, Bishop T, Papadakos N, Lui DF. Reducing radiation exposure and cancer risk for children with scoliosis: EOS the new gold standard. Spine Deform. 2023 Jul;11(4):847-851. doi: 10.1007/s43390-023-00653-6. Epub 2023 Mar 22. PMID: 36947393; PMCID: PMC10261215.
- Nishida M, Yagi M, Suzuki S, Takahashi Y, Nori S, Tsuji O, Nagoshi N, Fujita N, Matsumoto M, Nakamura M, Watanabe K. Persistent low bone mineral density in adolescent idiopathic scoliosis: A longitudinal study. J Orthop Sci. 2023 Sep;28(5):1099-1104. doi: 10.1016/j.jos.2022.07.005. Epub 2022 Aug 16. PMID: 35985936.
- Nandoliya KR, Sadagopan NS, Alwakeal A, Kemeny H, Cloney M, Dahdaleh NS, Koski T, El Tecle N. Adolescent Idiopathic Scoliosis and Pregnancy. Cureus. 2023 Oct 10;15(10):e46782. doi: 10.7759/cureus.46782. PMID: 37954752; PMCID: PMC10633849. “...Conclusions Patients with AIS had comparable rates of c-section to the general population, and even among patients with AIS, a history of spinal fusion was not associated with an increased incidence of c-section. Adolescent idiopathic scoliosis may be associated with difficulty administering anesthesia in a minority of patients, which can lead to a lower rate of combined spinal and epidural anesthesia usage. Furthermore, most patients with AIS will experience increased back pain during and after pregnancy. Changes in Cobb angle are seen in many patients, but the clinical significance of these changes remains unknown....”
- de Groot C, Heemskerk JL, Willigenburg NW, Altena MC, Kempen DHR. Educating Parents Improves Their Ability to Recognize Adolescent Idiopathic Scoliosis: A Diagnostic Accuracy Study. Children (Basel). 2022 Apr 15;9(4):563. doi: 10.3390/children9040563. PMID: 35455607; PMCID: PMC9025014."...Conclusions: This study showed that the education of parents improved their ability to detect scoliosis from 68.8% to 74.0%, without increasing the false positive referral rate...education can improve the awareness and ability to detect scoliosis, but will not replace screening by professionals. Education of the parents could be a strategy to facilitate adequate referral of patients with scoliosis to a physician in healthcare systems without professional screening."
- From trusted sources, for more information refer also to our website pages:
Scoliosis Support & Resource Groups for Parents and Patients
(the following pages are intended primarily to educate health professionals and public health policy officials)
Links to Media Coverage and Publications reporting on the state (crisis) of Scoliosis care in Canada.
Links to AIS references, including Publications on Curve Progression and Bone Density/Osteopenia.
Links to the Impact Adolescent Idiopathic Scoliosis (AIS) has on children
Links to Articles and Published studies on the Conseqences of Not Screening for Scoliosis and Delays to Surgery.
Links to Publications on the Long-term Impact of Adolescent Idiopathic Scoliosis (AIS) into Adulthood
Conservative (non-operative) Treatment of Adolescent Idiopathic Scoliosis (AIS) in Children (Links to PSSE and Orthotic Bracing evidentiary studies)
Links to Paediatric Spinal Deformity Surgery (for AIS) (aka complex spine surgery) including risks and complications.
Links to Current Research Publications.
Links to School Screening Guideline publications, management articles, school screening studies, diagnostic tools and more.
Contact us at: CSSC@scoliosiscanada.ca
(Disclaimer: The non-profit Canadian Scoliosis Screening Coalition (CSSC) does not endorse any treatments, procedures, products, or health professionals referenced herein and referenced on our social media posts and in our webinars. This website's content and all referenced herein including content on our social media posts and in our webinars, is for information and educational purposes only and does not represent medical advice. CSSC is not responsible for material from linked sites and presence of such a link does not constitute an endorsement by CSSC of material on the linked site.)
©2025CanadianScoliosisScreeningCoalition ©2026CanadianScoliosisScreeningCoalition